

A Pancreatic Primer for Pancreatic Cancer Awareness Month
Though pancreatic cancer is considered rare, it is the fourth leading cause of cancer death and has the highest mortality rate of major cancers. For Pancreatic Cancer Awareness Month, let’s explore the pancreas and discuss why pancreatic cancer is such a challenge to treat.
History of Treatment
Pancreatic cancer was first described in 1761 by Italian anatomist Giovanni Battista Morgagni, considered to be the founder of modern anatomical pathology. In 1858, notable American Civil War physician and medical instructor Jacob Mendez Da Costa reexamined Morgagni’s findings and described the first microscopic diagnosis of pancreatic cancer.
The sterility and anesthetics of modern surgery allowed for the development of the pancreaticoduodenectomy, the most common pancreatic cancer surgery. It was first performed in 1898. In 1935, Allen Oldfather Whipple was the first American surgeon to perform the pancreaticoduodenectomy, which he popularized, and now it is commonly referred to as the Whipple procedure.
The Whipple procedure has remained the same at its core, though there have been some modifications made over the years. Currently, the five-year survival rate after a Whipple procedure is 20-25%. In comparison, the five-year survival rate for all stages of pancreatic cancer combined is 10%.
The Healthy Pancreas
The pancreas is a tadpole-shaped organ that is located at the back of the abdomen and is made up of small glandular clusters of epithelial cells. It consists of a head, body, and tail, with the head connected to the duodenum.
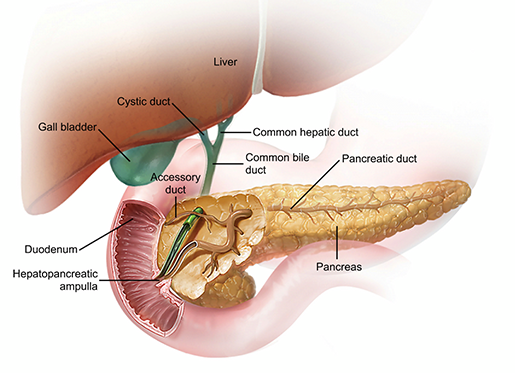
The pancreas, liver, gallbladder, and ducts. Image from Anatomy & Physiology.
The pancreas helps convert food into fuel for body cells. Its exocrine cells produce enzymes that, combined with electrolytes and water, make up a digestive fluid called pancreatic juice. That juice is carried through a system of ducts, and the common bile duct and pancreatic duct merge to form the ampulla of Vater, located in the duodenum. When pancreatic juice reaches the small intestine, it promotes digestion by breaking down sugars, fats, and starches.
The pancreas is also home to hormone-producing cell clusters known as islet cells. These clusters produce alpha cells and beta cells, which synthesize glucagon and insulin, respectively. Insulin and glucagon regulate the body’s glucose levels.
Insulin lowers blood glucose levels, signaling cells to convert glucose into energy or substances like glycogen and fats. Glucogen works primarily in the liver to promote the breakdown of glycogen into glucose, the synthesis of glucose from lactic acid and noncarbohydrate molecules, and the release of glucose to the blood.
Types of Pancreatic Cancer
There are two categories of pancreatic cancer: exocrine tumors and neuroendocrine tumors. Exocrine tumors begin in the cells that produce enzymes for digestion while neuroendocrine tumors begin in the cells that produce blood sugar-regulating hormones.
Adenocarcinoma is an exocrine tumor and is by far the most common type of pancreatic cancer, accounting for around 90% of all pancreatic cancers. The cancer usually starts in the pancreas’s ducts. Adenocarcinoma is not unique to the pancreas; it begins in the glands that line organs and can occur in the lungs, colon, esophagus, and other organs.
Pancreatic adenocarcinoma is most often found in the head of the pancreas. Often, the first symptom of a head tumor is jaundice, a yellowing of the eyes and skin. Jaundice is caused when a blockage of the common bile duct stops bile from entering the liver, causing a buildup of bilirubin.
Since the head of the pancreas is close to the common bile duct, tumors can press upon the duct. Adenocarcinoma that originates in the tail of the pancreas does not put pressure on the common bile duct until it has spread throughout the pancreas, and by that time the cancer has usually spread to other organs.
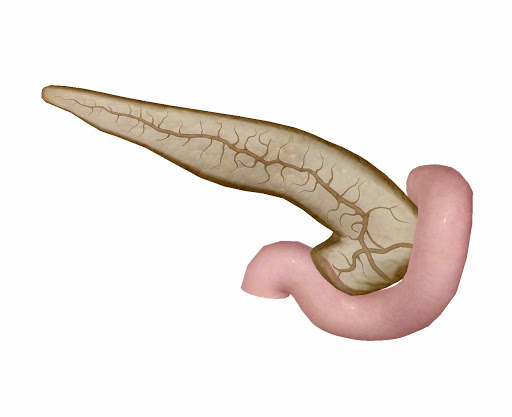
The pancreas (posterior view), its ducts, and the duodenum. Image from Human Anatomy Atlas.
Pancreatic neuroendocrine tumors (PNETs) make up around 5% of pancreatic cancers. Also known as islet cell tumors, PNETs can be either functional or nonfunctional. A functional PNET produces extra hormones, while a nonfunctional PNET does not. A nonfunctional PNET is more likely to be malignant.
Symptoms of a functional PNET can depend on the type of hormone the PNET makes—for example, a gastrinoma generates extra gastrin and might cause stomach ulcers, gastroesophageal reflux, or diarrhea.
However, many patients do not have these symptoms, and these tumors are often found through imaging studies like CAT scans performed to address other health issues. A biopsy confirms the diagnosis.
Screening and Risk Factors
Pancreatic cancer tends to develop after the age of 45, with 97% of cases occurring in that age group.
The risk factors associated with pancreatic cancer are nonspecific and are associated with other health problems. The highest risk factor is smoking. Other factors include diabetes, chronic pancreatitis, and a family history of pancreatic cancer. Several genetic syndromes increase the likelihood of pancreatic cancer, such as BRAC2 mutations and Peutz-Jeghers syndrome.
Because the majority of these risk factors are vague, people with family histories of pancreatic cancer are often the only group recommended for screening, despite the fact that hereditary pancreatic cancer accounts for only 10% of cases.
Researchers have found screening for pancreatic cancer to be a challenge, as the leading biomarker is not considered reliable. This biomarker is the tumor marker protein CA 19-9, and though people with pancreatic cancer are more likely to have more of CA 19-9 in their blood, increased levels of CA 19-9 can also be a sign of other illnesses, like gallstones. Instead of being used for screening, CA 19-9 blood tests are more often used to measure effectiveness of pancreatic cancer treatment.
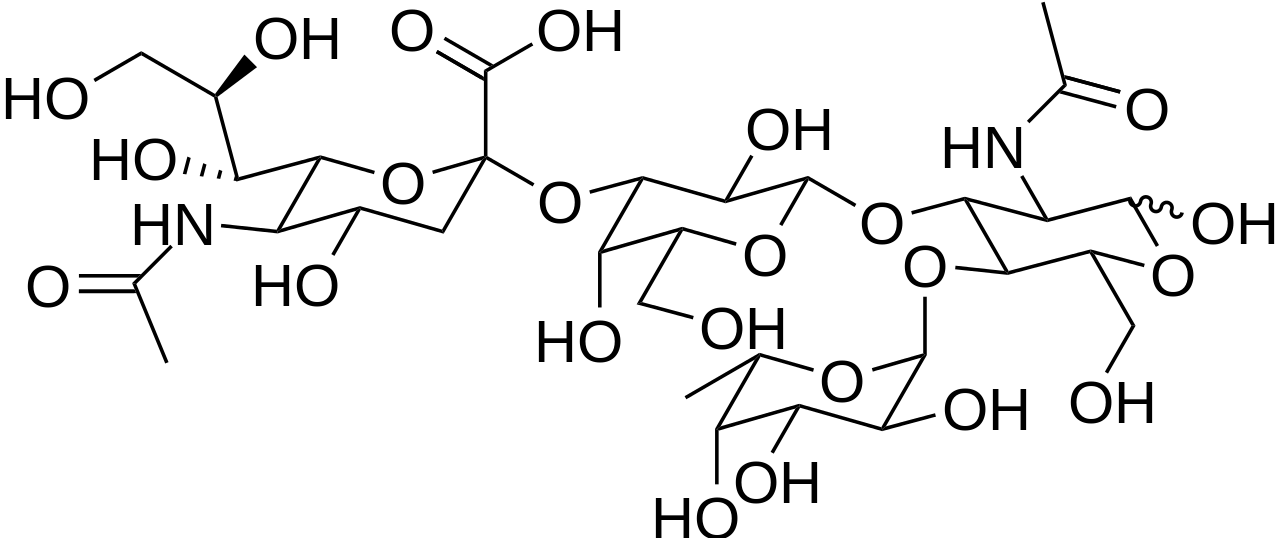
The chemical structure of CA 9-19. Image from Wikipedia Commons.
Imaging systems can be used to identify tumors, but their expense and invasive nature can be a barrier. Abdominal ultrasound is the easiest method, but pancreatic cancer is difficult to detect this way because of where the pancreas is located in the abdomen. Endoscopic ultrasound is the best option because it can also biopsy pancreatic tissue.

The pancreas in context. Image from Human Anatomy Atlas.
Why Is Pancreatic Cancer So Deadly?
Many complex factors compound to make pancreatic cancer one of the deadliest cancers.
Since there are few ways to screen for pancreatic cancer and patients tend not to exhibit symptoms until the cancer is advanced, it is difficult to catch pancreatic cancer in its early stages.
Treatment for pancreatic cancer includes radiation and chemotherapy as well as the Whipple procedure we mentioned earlier. This complex surgery takes 5-7 hours to complete: the surgeon removes the head of the pancreas, the first segment of the small intestine (the duodenum), part of the common bile duct, and the gallbladder. The surgeon then connects the remaining parts.
 Image from Shutterstock.
Image from Shutterstock.
Since, in the majority of cases, pancreatic cancer has spread beyond the pancreas by the time it is diagnosed, surgery is not typically effective in removing the cancer completely.
Chemotherapy drugs are not as effective against pancreatic cancer because pancreatic tumors are surrounded by nonmalignant cells, which prevents the chemotherapy from reaching them. Some drugs attempt to target specific parts of pancreatic cancer cells, but because pancreatic cancer is caused by many different mutations, it is difficult to develop effective drug therapy.
Conclusion
The pancreas produces a digestive fluid and contains islet cells that synthesize glucagon and insulin. Pancreatic cancer tends to either originate in the ducts (adenocarcinoma) or from the islet cells (PNETs).
Because of its nonspecific risk factors, a lack of distinct early symptoms, and inefficient screening methods, many people with pancreatic cancer are not diagnosed until the cancer has spread to other organs. Combined with the cancer’s resistance to chemotherapy, this means that current treatment for pancreatic cancer is not as effective as treatment for other cancers.
Despite these challenges, medical researchers are working on new imaging techniques, chemotherapies, immunotherapies, and other methods to fight pancreatic cancer. With more awareness and research, new treatments can be developed to improve prognosis.
Be sure to subscribe to the Visible Body Blog for more anatomy awesomeness!
Are you an instructor? We have award-winning 3D products and resources for your anatomy and physiology course! Learn more here.

{kind=link}